

{kind=link}
Think a morning cough is just something smokers live with?
It can be a warning sign your lungs are trying to clear out years of smoke.
A smoker’s cough often starts dry and harsh, then becomes phlegmy, worse in the morning and tied to chest tightness or shortness of breath.
This article walks through the common symptoms, how a smoker’s cough differs from a cold, what causes it, and when to seek prompt medical care.
Know the signs so you can act early.
Key Symptoms That Define a Smoker’s Cough

Smoker’s cough usually starts dry and harsh, then turns phlegmy over time. That shift happens because smoke toxins cause mucus to build up in your airways. The cough feels “hacky” and brings up sputum that varies in color and thickness. It’s not just a throat tickle. This comes from deep in your chest.
You’ll notice it’s worse first thing in the morning, then gets better as the day goes on. That’s because mucus pools in your airways overnight when you’re lying flat. Once you’re up and moving, gravity and activity help drain some of that buildup. The cough starts in your lower respiratory tract (lungs and bronchial tubes), not your throat.
Other stuff often shows up too. You might hear crackling or rattling when you breathe, feel chest tightness, or get short of breath doing normal things. Some people get a sore throat from all the coughing and irritation.
Common symptoms:
- Cough that sticks around for weeks or months
- Phlegm that’s white, yellow, green, or streaked with blood
- Mornings are noticeably worse
- Crackling or wheezing sounds
- Chest congestion or tightness
- Hard to catch your breath during physical stuff
How Smoker’s Cough Differs From Other Cough Types
Smoker’s cough develops in your lower airways and lungs. Coughs from colds or allergies start in your throat and upper respiratory tract. Duration’s another giveaway. Smoker’s cough lasts weeks to months and shows up most days, while a cold-related cough clears up in a week or two. Smoker’s cough also follows a pattern: bad in the morning, better by afternoon as mucus drains.
Infectious coughs bring fever and follow specific patterns. A continuous infectious cough means coughing hard for over an hour straight, or three or more coughing episodes in 24 hours. If you’ve got a new cough plus fever, you’re probably dealing with an infection (COVID-19, flu, bronchitis) rather than smoking irritation.
| Cough Type | Defining Features |
|---|---|
| Smoker’s cough | Starts in lower airways, lasts weeks to months, brings up phlegm, worse in morning, gets better through the day |
| Cold or infection cough | Starts in throat, lasts 1 to 2 weeks, often includes fever, continuous episodes (over 1 hour or 3+ times in 24 hours) |
| Allergy cough | Triggered by specific allergens, usually dry, comes and goes with exposure, no fever or colored mucus |
What Causes Smoker’s Cough and Airway Symptoms

Tobacco smoke has toxins that paralyze tiny hair-like structures called cilia lining your airways. Normally, cilia sweep mucus and debris up and out of your lungs in a constant cleaning motion. When smoke slows or stops that process, mucus piles up. Your body coughs to try clearing it out.
The constant irritation causes inflammation throughout your airways. Your bronchial tube lining swells and makes even more mucus, creating a cycle that makes everything worse. After you quit, it can take weeks to months for cilia to recover. During recovery, you might actually cough more as the cilia start working again and push out accumulated mucus.
Long-term smoking raises your risk for serious respiratory problems. Chronic bronchitis (persistent airway inflammation) and COPD (chronic obstructive pulmonary disease) are common complications. Smoking also increases your risk for lung infections like pneumonia and bronchitis, plus significantly raises the chance of lung cancer. COPD is progressive, meaning it gets worse over time. It can be managed but not cured.
Smoker’s Cough Symptoms That Suggest COPD

What starts as a simple smoker’s cough can turn into COPD if smoking continues. Symptoms don’t jump overnight. They creep up slowly, so you might write off increasing breathlessness or daily coughing as “normal for a smoker.” But persistent, daily symptoms aren’t normal and need medical evaluation. If your cough’s been around for months or years and you’re also noticing that climbing stairs or carrying groceries leaves you winded, the damage may have gone beyond simple irritation.
Symptom severity with COPD fluctuates. Some days breathing feels easier. Other days even talking takes effort. This variability is typical and doesn’t mean the condition’s going away. If your symptoms are getting worse over weeks or months (you need to stop and rest more often, usual activities now trigger shortness of breath), that progression matters clinically and should be checked.
Red flags include coughing up blood, chest pain that won’t ease, or feeling breathless even sitting still. If mucus production increases or changes color (especially to dark yellow, green, or blood-tinged), or if you’re losing weight without trying, see a clinician soon. COPD affects not just your lungs but your overall energy and quality of life, so early diagnosis helps you start treatment before symptoms become disabling.
Key COPD Symptoms
The three hallmark symptoms are persistent shortness of breath, chronic cough, and wheezing or chest tightness. Shortness of breath (also called dyspnea) may feel like you can’t catch your breath, like your chest is heavy, or like you’re gasping for air. It can be triggered by activity or happen even at rest as the disease gets worse. Chronic cough in COPD is present most days and may be productive (bringing up sputum, a mix of saliva and mucus) or dry. Wheezing happens when narrowed airways create a whistling sound during breathing. Chest tightness can range from mild pressure to painful constriction that makes each breath uncomfortable. Additional progression signs include coughing up blood (hemoptysis), recurring respiratory infections, persistent chest discomfort, and increasing difficulty with daily tasks that used to be manageable.
Diagnostic Steps for Persistent Smoker’s Cough Symptoms

If you see a doctor about a long-lasting cough, they’ll start with questions. Your smoking history, how long you’ve had the cough, what the mucus looks like, whether you’ve noticed shortness of breath or chest pain. They’ll listen to your lungs with a stethoscope to check for wheezing, crackling, or reduced airflow. Depending on what they hear and your answers, they may order tests to figure out what’s causing symptoms and how much lung function you still have.
The most common test is spirometry, which measures how much air you can blow out and how quickly. You breathe into a mouthpiece connected to a handheld device, and the results show whether your airways are narrowed or blocked. Other tests may include a chest X-ray to look for lung damage or infection, pulse oximetry (a small clip on your finger that measures oxygen levels), or a sputum culture to check for bacteria if infection’s suspected. If there are concerning signs like blood in your mucus or unexplained weight loss, your doctor may arrange lung cancer screening.
Common diagnostic tools:
- Spirometry (breathing test for lung capacity and airflow)
- Chest X-ray (imaging to check for lung damage, infection, or masses)
- Pulse oximetry (measures oxygen saturation in your blood)
- Sputum culture (tests mucus for infection)
- CT scan or lung cancer screening (if red-flag symptoms are present)
When Smoker’s Cough Symptoms Require Medical Attention

Any cough lasting more than 3 weeks should be checked by a doctor. A cough that hangs around that long isn’t “just a cough.” It’s a signal that something in your respiratory system needs attention. Even if you’re still smoking and think the cough is expected, a medical evaluation can catch early signs of COPD, chronic bronchitis, or other treatable conditions before they progress.
Some symptoms need same-day or emergency care. Don’t wait if you’re experiencing any of the warning signs below. These can point to serious complications like a lung infection, blood clot, collapsed lung, or cancer. Delaying care can be dangerous.
Seek urgent medical attention if you have:
- Coughing up blood (even small streaks or spots)
- Severe chest pain or new, sharp pain in your ribs
- Shortness of breath at rest or breathlessness that’s rapidly getting worse
- Persistent headaches that don’t respond to usual treatment
- Unexplained weight loss (losing weight without trying or changing your diet)
Treatment and Home Relief Strategies for Smoker’s Cough

Medical treatment depends on the underlying cause and severity. If airway inflammation or early COPD is involved, doctors may prescribe bronchodilators (medications that relax the muscles around your airways to make breathing easier) or inhaled corticosteroids (anti-inflammatory medications that reduce airway swelling). These are usually delivered through an inhaler. If mucus is thick and hard to cough up, mucolytics (medications that thin mucus) may help. Cough suppressants are sometimes used, but only in specific situations. Suppressing a productive cough can actually make things worse by trapping mucus in your lungs.
Some symptoms respond well to targeted medications. If you have a bacterial infection on top of your smoker’s cough, antibiotics may be needed. Oxygen therapy may be recommended if your blood oxygen levels are low, especially during sleep or physical activity. The key is getting an accurate diagnosis first, because treating the wrong thing won’t help and may delay the care you actually need.
Home-relief strategies can ease symptoms while you’re working on quitting or waiting for medical treatment to take effect. These won’t cure the underlying problem, but they can make day-to-day breathing and coughing more comfortable. Start with these measures, but if symptoms don’t improve within a few weeks or they get worse, it’s time to see a clinician rather than continuing to self-manage.
If you’ve tried home remedies for more than 3 weeks without improvement, or if you develop new symptoms like fever, blood in mucus, or worsening shortness of breath, switch from self-care to medical treatment. Home strategies are supportive, not curative. They work best for mild symptoms or as a complement to prescribed treatment.
Six at-home relief strategies:
- Drink plenty of water throughout the day to thin mucus and keep airways moist
- Use a humidifier or take steamy showers to add moisture to the air and loosen mucus
- Elevate your head with an extra pillow when sleeping to prevent mucus from pooling in your airways overnight
- Gargle with warm salt water several times a day to soothe throat irritation and reduce inflammation
- Use honey in herbal tea (honey’s a natural antibacterial and coats the throat) to ease soreness
- Avoid or limit dehydrating stuff like excess coffee and alcohol, which can thicken mucus
Symptom Improvement Timeline After Quitting Smoking
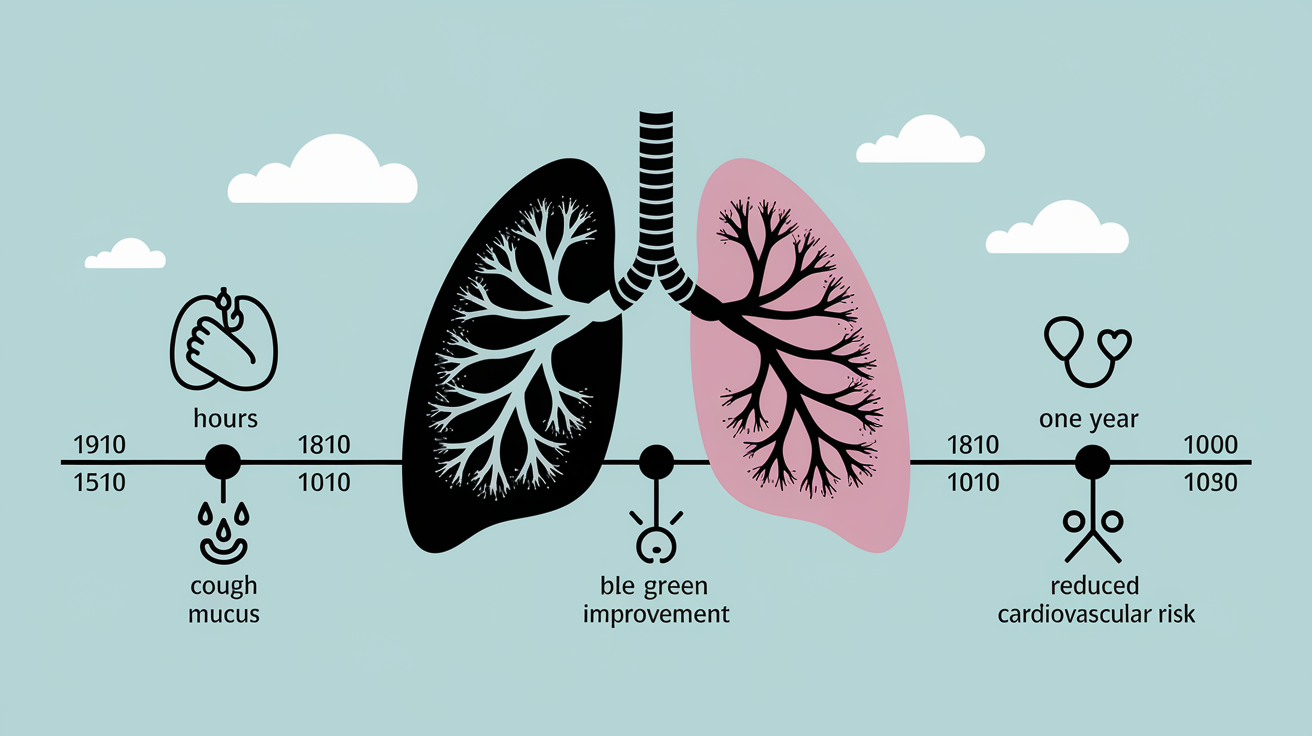
Quitting smoking is the only way to truly get rid of smoker’s cough. Medications and home remedies can help manage symptoms, but as long as you’re still inhaling smoke, the damage continues. The good news? Benefits start almost immediately after your last cigarette. Within hours, your body begins to repair itself. Lung function starts to improve within weeks.
Your cough may actually get worse in the first few weeks after quitting. That can be frustrating, but it’s a sign of healing. As cilia in your airways recover and start moving again, they push out the mucus and tar that built up while you were smoking. This temporary increase in coughing and mucus production usually peaks around 2 to 4 weeks, then begins to ease. Noticeable improvement in cough and shortness of breath typically happens within a few months. Most people see significant recovery within one year.
| Time After Quitting | What to Expect |
|---|---|
| First few weeks | Cough may worsen as cilia recover and begin clearing built-up mucus; increased mucus production is normal during this phase |
| 1 to 3 months | Cough and shortness of breath begin to improve; lung function increases; daily activities feel easier |
| One year | Significant improvement in respiratory symptoms; risk of heart disease drops by half; lung capacity continues to improve |
Final Words
We covered what a smoker’s cough looks like. It often starts dry, becomes phlegmy, is worse in the morning, and can come with wheeze, crackles, or blood-tinged sputum.
You learned how it differs from colds, what toxins do to airway cilia, which tests a clinician may use, and simple home steps plus medical treatments.
If you notice worrying or worsening smoker’s cough symptoms, such as a cough lasting more than three weeks, blood in mucus, severe breathlessness, or weight loss, seek care. Quitting smoking and getting timely help often lead to real improvement within months.
FAQ
Q: How do you know if you have a smoker cough?
A: You have a smoker’s cough if you’re a smoker with a persistent, harsh cough that often starts dry then becomes productive and is worse in the morning. Seek care if it lasts over 3 weeks or you cough blood.
Q: How do you get rid of a smokers cough?
A: You get rid of a smoker’s cough by quitting smoking—the only true cure. Short-term relief includes hydration, humidified air or steam, honey or lozenges; prescribed mucolytics or inhalers may help.
Q: What does a smoker cough sound like?
A: A smoker’s cough sounds raspy, hacky, or harsh and may be deep and phlegmy. It’s often worse in the morning and can include wheeze or crackling breath sounds.
Q: Will my cough go away if I stop smoking?
A: Your cough may improve if you stop smoking, but it can worsen for several weeks as cilia recover. Noticeable improvement often appears within months, with much recovery by one year for many people.