

{kind=link}
Think surgery is the last resort for heartburn? Not always.
If diet changes and medicines still leave you waking with chest burning or a sour taste, a surgical fix might restore normal digestion.
Surgery aims to repair the valve at the bottom of the esophagus (the tube from your mouth to your stomach) rather than only lowering acid.
This post explains the main procedures, fundoplication (full and partial wraps), the LINX magnetic device, and incisionless options like TIF, who may benefit, what recovery looks like, and the key risks and rewards to discuss with your doctor.
Understanding Available GERD Surgical Procedures

Surgery becomes an option when lifestyle changes and medications don’t control GERD symptoms. If you’ve adjusted your diet, propped up the head of your bed, tried multiple rounds of proton pump inhibitors, and still wake up with chest pain or that sour taste of regurgitation, your doctor might bring up surgical evaluation. It’s also considered when medication side effects start piling up, or when you’re just tired of taking pills every single day and want something more permanent.
Most GERD surgeries today use minimally invasive laparoscopic techniques. That means five small incisions in your abdomen instead of one big one. The two main surgical approaches are fundoplication and magnetic sphincter augmentation. Fundoplication wraps part of your stomach around the lower esophagus and stitches it there to reinforce the lower esophageal sphincter (LES), that valve meant to keep acid from flowing backward. Magnetic sphincter augmentation uses a small ring of magnetic beads placed around the LES to strengthen how it closes. Both are trying to restore the natural barrier between your stomach and esophagus.
Recovery’s typically quick. Most people spend one night in the hospital and get back to work in about two weeks. The goal is the same, reducing or stopping reflux by fixing the mechanical problem at the base of the esophagus instead of just turning down stomach acid with medication.
Main surgical options:
Nissen fundoplication – full 360 degree wrap around the esophagus
Toupet fundoplication – partial 270 degree wrap, often used when esophageal motility is weak
Dor fundoplication – anterior partial wrap for specific situations
LINX magnetic sphincter augmentation – magnetized ring device that opens and closes with pressure
Transoral incisionless fundoplication (TIF) – endoscopic procedure done through the mouth
Fundoplication Variants for GERD Treatment
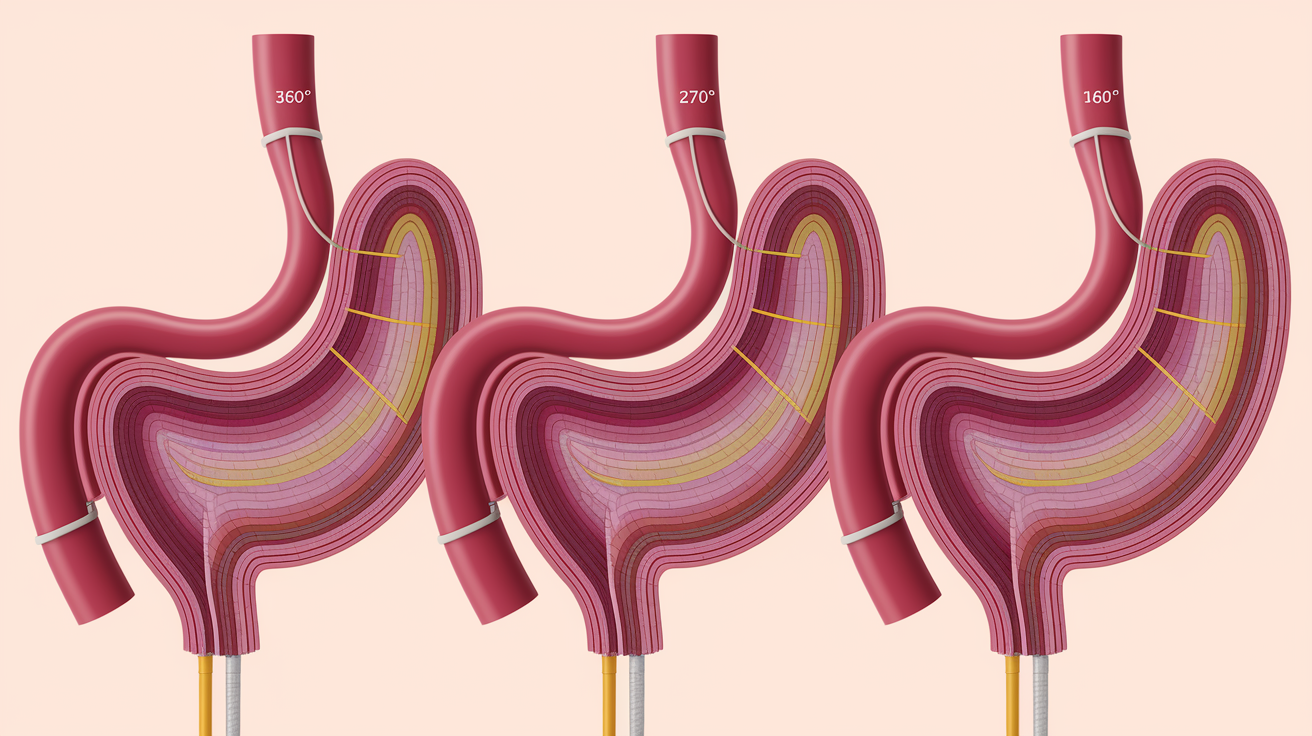
Different fundoplication techniques exist because patients aren’t identical. Your anatomy, symptom patterns, and how well your esophagus moves food all play into which approach makes sense. The degree of wrap, whether full or partial, affects how tightly the valve closes and how easily food can pass through. Surgeons pick the wrap style based on preoperative testing, especially measurements of how well your esophagus squeezes and pushes food downward.
Nissen Fundoplication
The Nissen fundoplication is the most widely performed anti-reflux surgery. Some call it the gold standard. A surgeon creates a 360 degree wrap by bringing the top of the stomach all the way around the lower esophagus and stitching it there. This reinforces the LES and creates a strong one way valve. The procedure is done laparoscopically, using five small keyhole incisions, a lighted camera, and tiny instruments. The full wrap gives excellent reflux control, but it can cause functional side effects like bloating, increased gas, and trouble belching because the valve is very tight. When food goes down, it stays down, and so does air.
Toupet Fundoplication
The Toupet fundoplication is a partial, posterior wrap covering about 270 degrees of the esophagus. It leaves the front of the esophagus unwrapped. This approach gets chosen when preoperative manometry shows weak or uncoordinated esophageal motility. A looser wrap cuts down the risk of postoperative swallowing problems, especially for patients whose esophagus already struggles to push food downward. Trade off is slightly less reflux control compared to a full Nissen wrap, but the reduced risk of dysphagia often makes it the better pick for the right patient.
Dor Fundoplication
The Dor fundoplication is an anterior partial wrap that folds the stomach over the front of the esophagus. It’s less commonly used but can be valuable after certain esophageal surgeries, like a Heller myotomy for achalasia, where the muscle at the bottom of the esophagus gets cut to relieve swallowing difficulty. The Dor wrap helps prevent reflux without creating too much resistance. It’s rarely the first choice for straightforward GERD, but it has a role in specific reconstructive scenarios.
| Wrap Type | Degree of Wrap | Typical Patient Profile |
|---|---|---|
| Nissen | 360° (full) | Strong esophageal motility, severe reflux |
| Toupet | 270° (posterior partial) | Weak esophageal motility, dysphagia risk |
| Dor | 180–200° (anterior partial) | Post-myotomy, reconstructive cases |
LINX Magnetic Sphincter Augmentation as a GERD Option

The LINX device is a small bracelet of magnetic titanium beads placed around the lower esophageal sphincter during a laparoscopic procedure. The magnets hold the beads together, keeping the sphincter closed at rest. When you swallow, pressure from food or liquid temporarily opens the magnetic ring, allowing passage into the stomach. Once the food passes, the magnets pull the beads back together, restoring the barrier.
Randomized controlled trials support using LINX for GERD, showing excellent reflux control and minimal side effects. One advantage over full Nissen fundoplication is that the LINX device allows venting. If pressure builds in your stomach, the ring can open slightly to let gas escape. This reduces the risk of postoperative bloating and the inability to belch, two common complaints after a 360 degree wrap. The surgeon customizes the device size to fit your anatomy during the operation.
Key benefits of LINX:
Preserves the ability to belch and vomit when needed
Shorter operative time compared to some fundoplication techniques
Minimal postoperative dietary restrictions in many cases
Supported by trial evidence showing durable symptom relief
Incisionless and Endoscopic GERD Procedures
Not all anti-reflux procedures need abdominal incisions. Endoscopic techniques access the esophagus and stomach through the mouth, no external cuts. These procedures appeal to patients who want to skip surgery but need more than medication alone. Transoral incisionless fundoplication, or TIF, is the most widely studied incisionless option.
Other endoscopic approaches, like the Stretta radiofrequency treatment, use heat energy to remodel the LES tissue. These procedures are generally done at specialized centers with advanced endoscopy programs. Outcomes vary, and not all patients are candidates, especially those with large hiatal hernias or severe esophageal damage.
TIF Procedure Overview
During TIF, a gastroenterologist or specially trained surgeon passes an endoscope through your mouth into your stomach. The endoscope carries a device that folds and fastens tissue at the gastroesophageal junction to recreate an anti-reflux valve. The procedure’s typically done under general anesthesia and can be performed on an outpatient basis. Candidates usually have small hiatal hernias, less than 2 centimeters, and symptoms that don’t respond well to medication. Larger hernias often require traditional surgical repair first.
| Procedure | Approach | Typical Candidate |
|---|---|---|
| TIF | Endoscopic, through the mouth | Small hernia, medication-refractory GERD |
| Stretta | Endoscopic radiofrequency | Mild to moderate reflux, no large hernia |
| Laparoscopic fundoplication | Five small abdominal incisions | Moderate to severe GERD, any hernia size |
Hiatal Hernia Repair and GERD Surgery Integration
A hiatal hernia happens when part of your stomach pushes up through the diaphragm into your chest. Many people with GERD also have a hiatal hernia, and the size affects which surgical option is best. Small hernias, typically under 2 centimeters, may not need repair, and some patients with small hernias are candidates for incisionless procedures like TIF. Larger hernias usually require surgical repair to prevent the wrap or device from slipping or failing.
Hernia repair’s often done at the same time as fundoplication or LINX placement. The surgeon reduces the stomach back into the abdomen and tightens the opening in the diaphragm, called the hiatus, by suturing the crural muscles together. This is known as cruroplasty. In some cases, especially when the hiatus is very wide, surgeons may use mesh to reinforce the repair, though many repairs are done with sutures alone.
Combining hernia repair with anti-reflux surgery addresses both the structural defect and the valve problem. Failing to repair a large hernia can lead to recurrent reflux or complications like wrap migration, where the fundoplication slips upward into the chest.
Preoperative Evaluation for GERD Surgery

Testing before surgery confirms that your symptoms are truly caused by reflux and makes sure your esophagus can tolerate the chosen procedure. Surgery without proper testing can lead to poor outcomes, especially if the real problem is something other than acid reflux.
Main preoperative tests:
Upper endoscopy (EGD) examines the lining of your esophagus and stomach, measures hernia size, and checks for complications like Barrett’s esophagus or strictures.
Esophageal manometry measures how well your esophagus squeezes and moves food. Weak motility may steer your surgeon toward a partial wrap instead of a full Nissen.
24 hour pH impedance monitoring tracks acid exposure in your esophagus over a full day and night. It confirms that acid is the main problem and shows how often reflux episodes occur.
Identifying the Right Surgery
Test results guide which procedure makes sense. A patient with normal esophageal motility and severe acid exposure on pH testing is a strong candidate for Nissen fundoplication or LINX. A patient with weak motility and moderate acid exposure may benefit more from a Toupet fundoplication. If manometry shows very poor esophageal function, surgery may not be safe, because a wrap could trap food and cause severe swallowing problems.
When Patients Are Not Candidates
Surgery isn’t recommended for everyone. Contraindications include very weak or absent esophageal motility (achalasia like patterns), active esophageal ulcers or infections, severe obesity without prior weight loss, and cases where symptoms aren’t clearly linked to acid reflux. Incomplete testing or testing that shows normal acid exposure may also rule out surgery, since the symptoms might be due to functional disorders rather than structural reflux.
Risks, Side Effects, and Complications Across GERD Surgeries

All surgical procedures carry risks. During laparoscopic GERD surgery, there’s a small chance of injury to nearby organs, including the liver, spleen, esophagus, or stomach. These injuries are rare but can require immediate repair or conversion to open surgery. Bleeding and infection are also possible, as with any operation.
Functional side effects are more common than serious injuries. After a full Nissen fundoplication, many patients experience gas bloat syndrome, difficulty belching or releasing gas, leading to bloating and discomfort after meals. Some patients have temporary trouble swallowing, called dysphagia, which usually improves over weeks to months as swelling resolves. A small number develop persistent dysphagia that may require dilation or, rarely, revision surgery. The inability to vomit is another consequence of a tight wrap, which can be distressing during a stomach virus.
Common complications and side effects:
Postoperative dysphagia (trouble swallowing)
Gas bloat syndrome and inability to belch
Increased flatulence
Inability to vomit
Wrap slippage or herniation into the chest
Recurrent reflux if the wrap loosens over time
LINX tends to have fewer bloating and belching side effects because the magnetic ring can open under pressure, but it carries its own risks, including device erosion into the esophagus in rare cases and the need for removal if problems occur.
Expected Recovery Timeline After GERD Surgery

Most patients spend one night in the hospital after laparoscopic fundoplication or LINX placement. Some centers discharge patients the same day if surgery’s done early and recovery is smooth. Pain is usually manageable with oral medication, and discomfort around the incision sites improves within a few days.
You’ll be encouraged to walk soon after surgery to reduce the risk of blood clots. Activity restrictions typically last two to four weeks. No heavy lifting over 10 to 15 pounds and no strenuous exercise. Most people return to work within about two weeks, depending on the physical demands of their job. Desk workers often go back sooner, while those in labor intensive roles may need three to four weeks.
Diet progression follows a careful timeline to allow healing:
Clear liquids for the first few days. Broth, water, juice, gelatin to minimize stress on the wrap.
Full liquids and pureed foods for the next one to two weeks. Smoothies, yogurt, mashed potatoes, scrambled eggs.
Soft foods for weeks three to four. Pasta, cooked vegetables, ground meat, soft bread.
Regular diet after four to six weeks, once swelling has fully resolved and the wrap has settled.
Long-Term Outcomes and Medication Use After Surgery

Many patients achieve excellent symptom relief after GERD surgery and can stop or significantly reduce their use of proton pump inhibitors. However, some continue to require medication, either right after surgery while swelling resolves or in the long term if reflux symptoms partially return. Clinical experience and published studies suggest that the majority of patients see substantial improvement.
Durability varies by procedure. Fundoplication has decades of follow up data showing that most wraps remain effective for many years, though a small percentage of patients experience wrap loosening or slippage over time. LINX is a newer device, so long term data beyond ten years is still accumulating, but trials show sustained reflux control in the majority of patients.
Long term considerations:
Some patients eventually restart low dose PPIs for occasional breakthrough symptoms.
Weight gain, pregnancy, or aging can increase intra-abdominal pressure and strain the repair.
Periodic endoscopy may be recommended to monitor for Barrett’s esophagus or other changes, especially if you had them before surgery.
Lifestyle habits still matter. Eating smaller meals, avoiding late night snacks, and managing weight help protect the surgical repair.
Revisional GERD Surgeries and Persistent Symptoms

A small percentage of patients develop recurrent symptoms after initial surgery. This can happen if the wrap loosens, slips upward into the chest, or was too tight to begin with, causing severe dysphagia. Revisional surgery, also called redo fundoplication, involves reopening the abdomen, taking down the original wrap, and creating a new one or repairing the hernia if it’s recurred.
Revisional procedures are more complex than primary surgeries because scar tissue makes dissection more difficult. Diagnostic testing is essential before planning a redo operation. Manometry, pH testing, and upper endoscopy help determine whether the problem is mechanical (a slipped wrap) or functional (poor esophageal motility that was missed the first time).
In some cases, the best option isn’t another fundoplication but removal of the wrap entirely, especially if esophageal motility has worsened. Patients considering revision should seek care at specialized centers with surgeons experienced in complex esophageal surgery, where multidisciplinary teams can review all options, including conversion to a different procedure or a return to medical management.
Comparing Surgical Options to Long-Term Medication Therapy
Surgery offers a durable anatomical correction. It fixes the valve and hernia rather than just suppressing acid production. Medications like proton pump inhibitors reduce symptoms but don’t repair the structural problem, so reflux continues even if you don’t feel it. Over time, ongoing reflux can lead to complications like strictures or Barrett’s esophagus, even on medication.
On the other hand, surgery carries upfront risks, requires recovery time, and may cause functional side effects. Some patients remain partially dependent on medication even after surgery, particularly if they have persistent low grade reflux or delayed gastric emptying. Long term medication use has its own concerns, including possible effects on bone density, nutrient absorption, and an increased risk of certain infections, though these risks are debated and not universally accepted.
| Option | Benefit | Limitation |
|---|---|---|
| Surgery | Restores anatomy, often reduces or eliminates meds, durable | Operative risks, recovery time, possible functional side effects |
| Medication (PPI) | Non-invasive, effective symptom control, easy to start and stop | Daily pill, does not fix valve, long-term cost and possible side effects |
Preparing for a GERD Surgery Consultation
Walking into a surgeon’s office prepared helps you make the best decision. Bring copies of any recent tests. Endoscopy reports, manometry results, and pH study summaries so the surgeon has a complete picture. If you’ve tried multiple medications, write down which ones you took, at what doses, and how well they worked. Note any side effects or concerns that pushed you toward considering surgery.
Specialized esophageal centers often combine gastroenterology and thoracic surgery in a single visit, letting you hear both medical and surgical perspectives before deciding. This multidisciplinary approach ensures you understand all your options, including whether optimizing medication therapy might still be worth trying.
Questions to ask during your consultation:
How many of these procedures have you performed, and what are your complication rates?
Which procedure do you recommend for me, and why?
What preoperative tests do I still need?
What are realistic expectations for symptom relief and medication use after surgery?
How long will recovery take, and what restrictions will I have?
What happens if the surgery doesn’t work or symptoms return?
Final Words
If surgery is on your list, this article walked you through the main choices—fundoplication variants, the LINX device, and incisionless options—plus how hiatal hernia repair fits in.
It also covered the tests surgeons use, realistic risks and recovery expectations, long-term results, when a redo may be needed, and how to prepare for a consult.
Use those testing and consult tips to ask the right questions and weigh benefits versus lifelong medicine. With careful evaluation and a good surgical team, many people find real relief from gerd surgical options and get back to normal life.
FAQ
Q: What is the best surgery for GERD?
A: The best surgery for GERD depends on your test results and goals. Common options are fundoplication (stomach wrapped around the esophagus to strengthen the lower esophageal sphincter) and LINX (magnetic ring).
Q: How painful is fundoplication surgery?
A: Fundoplication (stomach wrap) surgery pain is usually moderate for a few days, controlled with prescription pain medicine; most people switch to over-the-counter meds within a week and return to light activity in 1-2 weeks.
Q: What qualifies you for GERD surgery?
A: You qualify for GERD surgery if lifestyle changes and meds don’t control symptoms, testing (pH, manometry, endoscopy) shows reflux or dysfunction, or you have complications like esophagitis or a large hiatal hernia. Only a clinician can confirm.
Q: What are the drawbacks to fundoplication?
A: The drawbacks to fundoplication (stomach wrap) are possible swallowing trouble (dysphagia), gas-bloat and inability to belch or vomit, surgical risks like organ injury, and some patients may need revisional surgery.